Bodies: Solutions We Love
- The “Obesity Crisis” Is a Fatphobic Myth
- Share

Illustrations by Adobe Stock
The “Obesity Crisis” Is a Fatphobic Myth
Fatness is treated as a moral failure, but the facts show it is all systemic.
4 MIN READ
Nov 21, 2022
In the ’90s, the Centers for Disease Control and Prevention declared the United States was experiencing an “obesity crisis.”
At the time, CDC Director Jeffrey P. Koplan blamed fat people for this “rise in obesity,” saying that obese people needed to reduce their caloric intake and increase their physical activity, while those interacting with obese people needed to encourage them to do so. More than 30 years later, this guidance still informs how our society interacts with people deemed obese, defined as having a body mass index (BMI) number of 30 or higher. Rather than treating fatness as ordinary, it’s instead viewed as a moral failure. To be blunt: This is completely wrong.
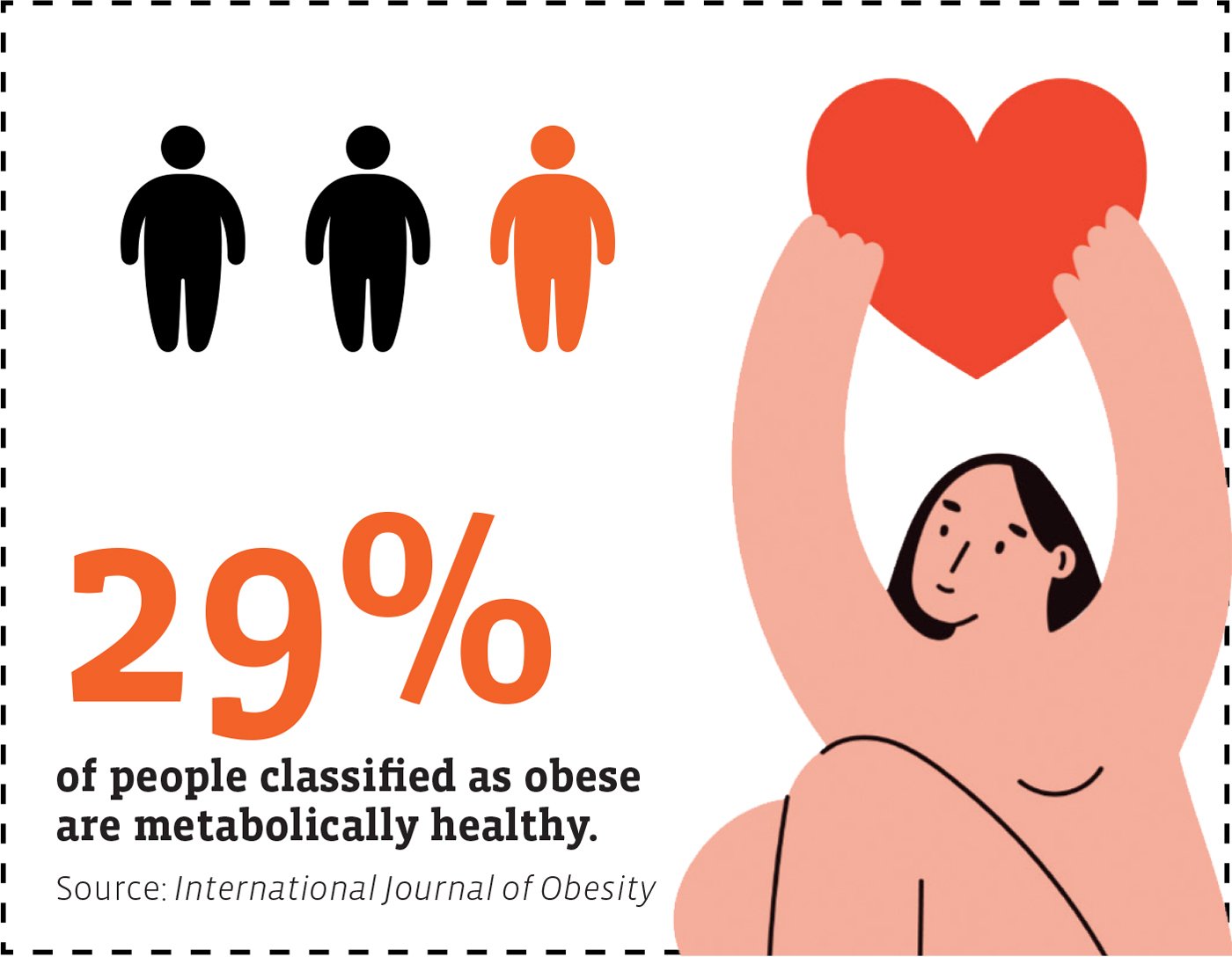
The BMI doesn’t adequately measure body fat. Rather than accounting for differences in racial demographics, body fat percentage, and body fat distribution, the BMI measures a person’s body fat by dividing their weight in kilograms by the square of their height in meters. Beyond that, 2 million Americans with a BMI over 35 are considered healthy. More than 30 million people classified as “overweight” are actually healthy, as are an additional 19.8 million deemed “obese.”
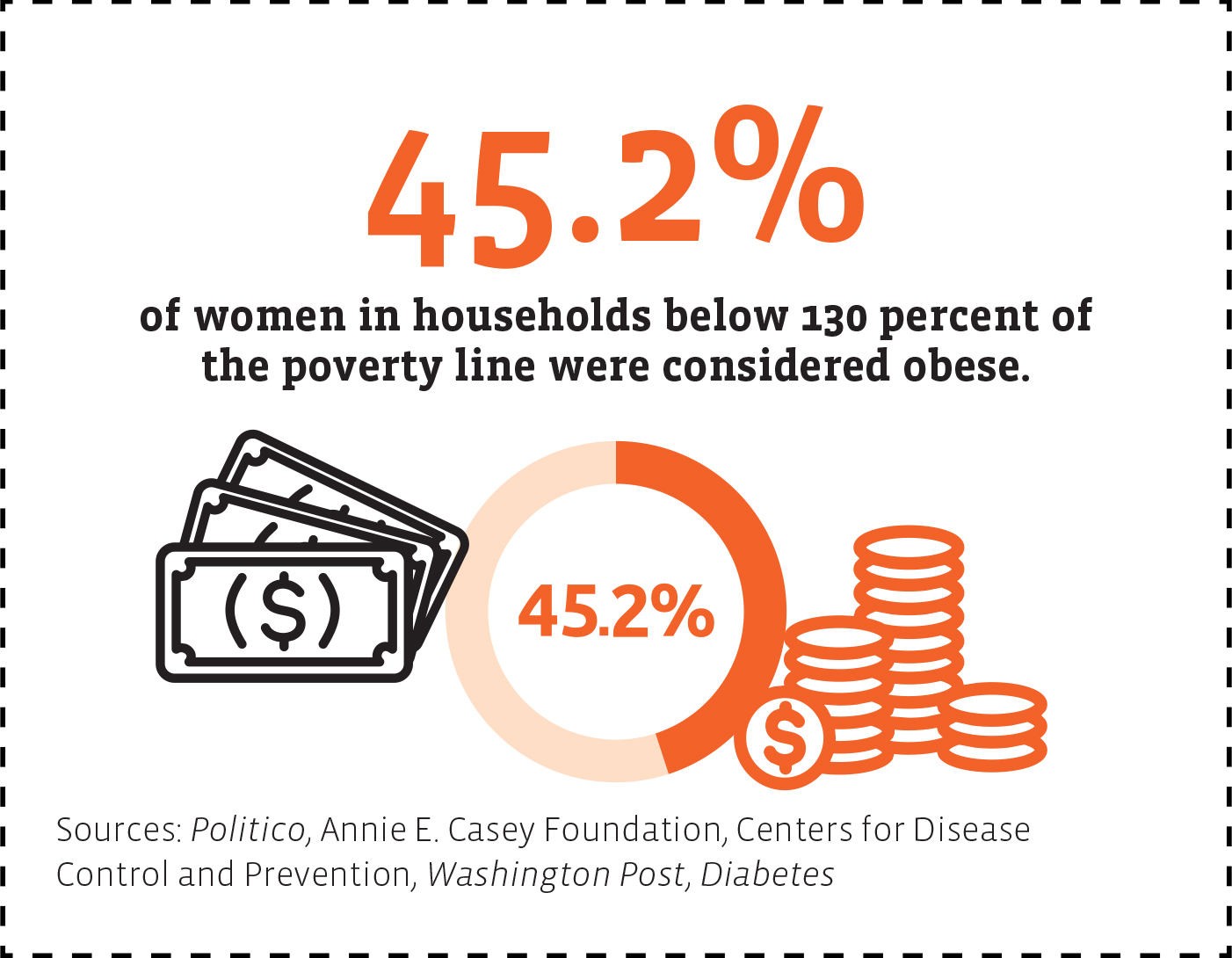
Federal agencies aren’t investing much in nutrition research. In 2019, Politico found that the budgets for federal nutrition programs have remained stagnant for the last three decades. In 2018, the National Institutes of Health invested $1.8 billion in nutrition research, less than 5% of its annual budget. There’s also a clear link between poverty and obesity, and federal programs that provide impoverished Americans with funds to aid nutrition actually contribute to obesity. More than 41 million people in the U.S. received benefits from the Supplemental Nutrition Assistance Program (SNAP) in 2021, which is designed to assist with food insecurity. Yet the SNAP program has been associated with poorer cardiometabolic health among children and adults. Nearly half of women in households with incomes below 130% of the federal poverty line (the criteria for SNAP) were obese between 2011 and 2014. U.S. counties with poverty rates of more than 35% have obesity rates 145% higher than wealthy counties.
Diets don’t work, so advising fat people to “lose weight” isn’t a viable solution. While more than one-third of people in the U.S. are dieting at any given time, they’ll likely regain the weight they’ve lost within a year. Roughly 80% of people who shed a significant amount of weight will regain it in two years.
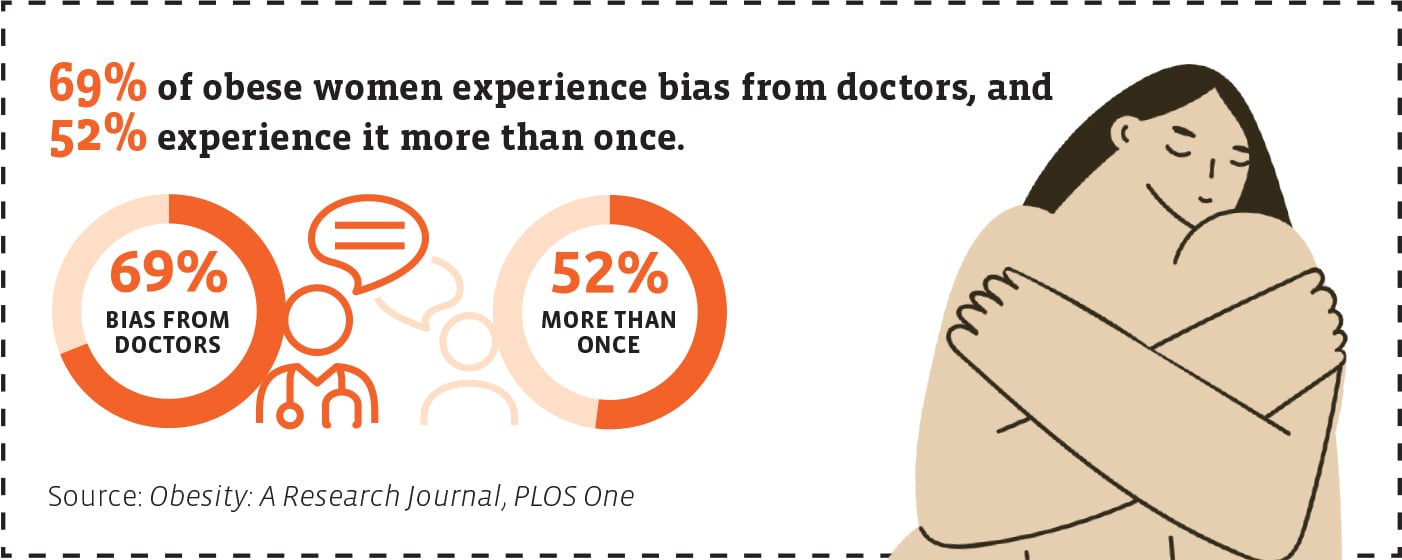
Doctors harbor fat bias, which prevents fat people from receiving adequate care. In 2009, Rudd Center for Food Policy and Health scholars Rebecca M. Puhl and Chelsea A. Heuer surveyed 2,449 fat women for a study about fat bias among health care professionals. They found 69% of those surveyed experienced bias from doctors while 52% endured recurring fat bias. A subsequent 2012 study found strong implicit and explicit anti-fat bias among physicians.
![Infographic text reads: Patients with shortness of breath who are obese are told to change lifestyle 54% [of the time]. Patients who are not obese being told so: 13%. Patients who are obese receiving medication to manage symptoms: 5%. Patients who are not obese receiving medication: 23%. Sources: American Journal of Preventative Medicine, Obesity Reviews, Patient Education and Counseling, International Journal of Obesity.](https://www.yesmagazine.org/wp-content/uploads/2022/11/Stat7.jpg)
Weight bias in all these areas only leads fat people to eat more to cope with the stigma directed at their bodies. In a 2006 Obesity study, 79% of respondents said they used food to cope with weight stigma on multiple occasions. Ninety percent used food to cope with weight bias at least once, and 80% of respondents ate more food to cope at least once.
If we want to lower rates of “obesity” in the United States, let’s start with addressing the systemic issue fueling the problem: fatphobia.

|
Evette Dionne
is the executive editor at YES! Media, where she leads YES! Magazine. She is the former editor-in-chief at Bitch Media, and an award-winning journalist, pop culture critic, and magazine editor who covers culture and politics through the lenses of race, gender, class, and size. Her newest book, Weightless: Making Space for My Resilient Body and Soul, was published in December 2022 by Ecco. She’s also the author of Lifting As We Climb, which was longlisted for a National Book Award and won a Coretta Scott King author honor. Evette is based in Denver, and speaks English.
|
Reprints and reposts: YES! Magazine encourages you to make free use of this article by taking these easy steps.